
 Optimising breast shape with auto augmentation
Optimising breast shape with auto augmentation
ARTICLES
Understanding the Placement of Breast Implants in Relation to the Pectoral Muscles
Breast augmentation involves the placement of breast implants to enhance the size, shape, and overall appearance of the breasts. One critical factor to consider during breast augmentation is the placement of the implants relative to the pectoral muscles. This decision plays a vital role in achieving the desired aesthetic outcome and ensuring long-term satisfaction for patients. In this article, I will explain the different placement options and their implications, providing you with a comprehensive understanding of the relationship between breast implants and the pectoral muscles.
The Anatomy
When a pocket is dissected by the surgeon to place a breast implant, it is usually in a natural interface between tissues known as a ‘plane’. Various different planes have been used for breast augmentation, each of which have advantages and disadvantages. It’s vitally important to understand the relationship of the pectoral muscle relative to the breast gland (shown below) to fully understand these planes.

Anatomical arrangement of the pectoral muscles and breast tissue. The white line represents the fascial layer that overlies the pectoral muscles.
Understanding breast implant placement: sub-glandular, sub-muscular or somewhere between.
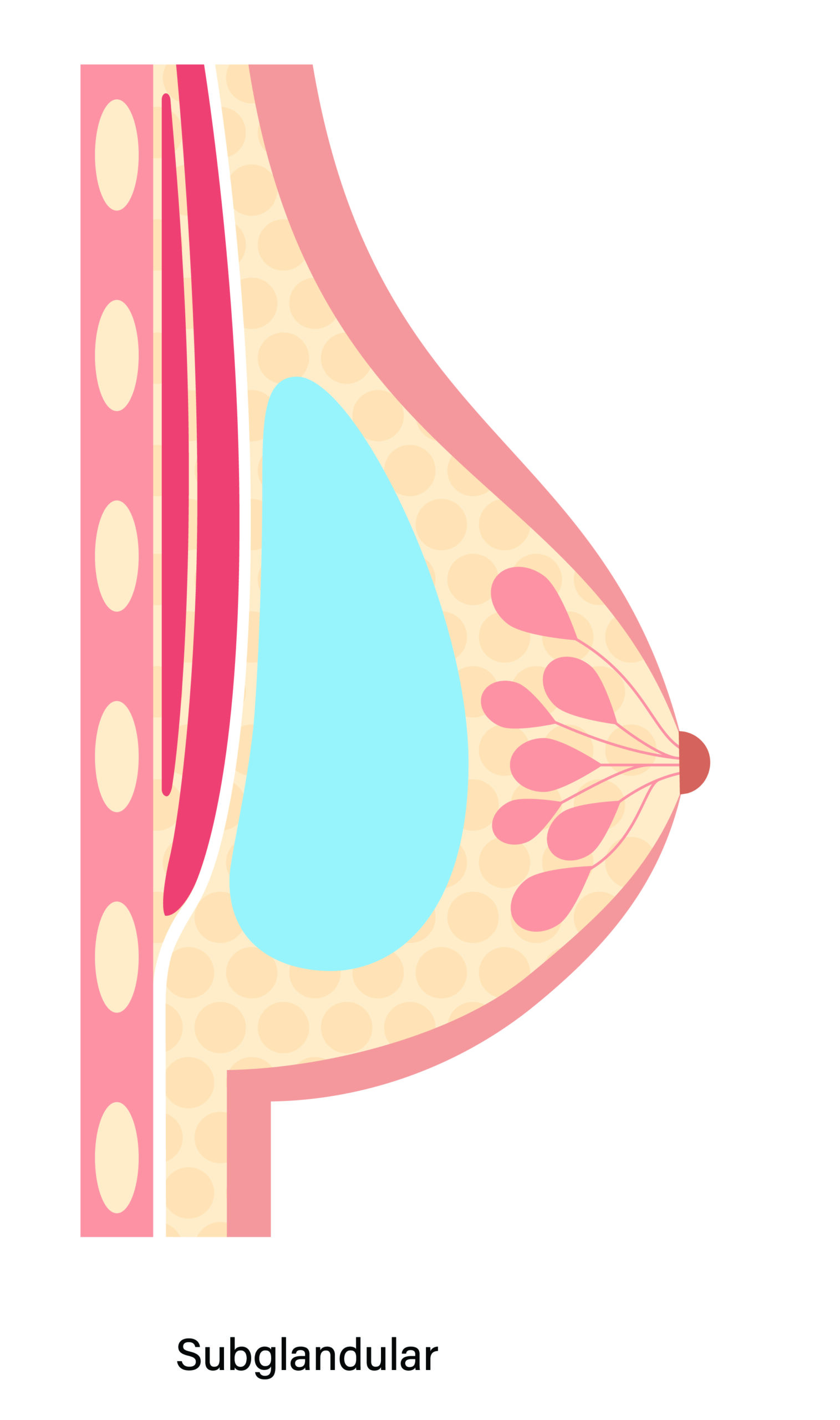
1. Sub-glandular placement
The sub-glandular plane is also referred to as sub-mammary or pre-pectoral. This is the original plane described for the placement of implants. In this plane the implant sits against the under surface of the breast and on top of the pectoral muscles.
One significant advantage of sub-glandular placement is the potentially shorter and less painful recovery period. Since the pectoral muscles remain untouched during the procedure, patients may experience less discomfort and a quicker return to normal activities.
Another advantage of the sub-glandular plane is that the implant fills out the breast fully and is not restricted by the muscle movement or anatomy. It offers greater flexibility for a more accurate placement to enhance the central cleavage area or the outer parts of the breast. The true dimensions of the implants are also much more directly impacted on the breast shape. Hence, I believe that shaped or anatomical implants (also called tear-drop) are better placed in the sub-glandular plane. When round implants are used in the sub-glandular plane, they may appear more projected in the upper half, which some patients desire.
The disadvantage of the sub-glandular plane is that, if there is not very much breast tissue then the edge of the implant can be visible. Thinned tissues can also allow the ripples on the implant surface to show through to the breast. When using smooth surfaced implants (see article on textured or smooth surface implants), there also appears to be a higher capsular contracture rate in this plane. Hence, in my practice, if the patient and I decide to use the sub-glandular plane, I will often recommend textured implants.
Some patients worry that placing the implant directly under the breast might interfere with mammographic readings and breast cancer detection, although there is little scientific evidence for this, especially using modern radiographic machines and techniques.

Shaped or anatomical implants are best used in the sub-glandular plane. When placed in the sub-muscular plane the upper sloping edge is not fully appreciated because of the bulge of the muscle.
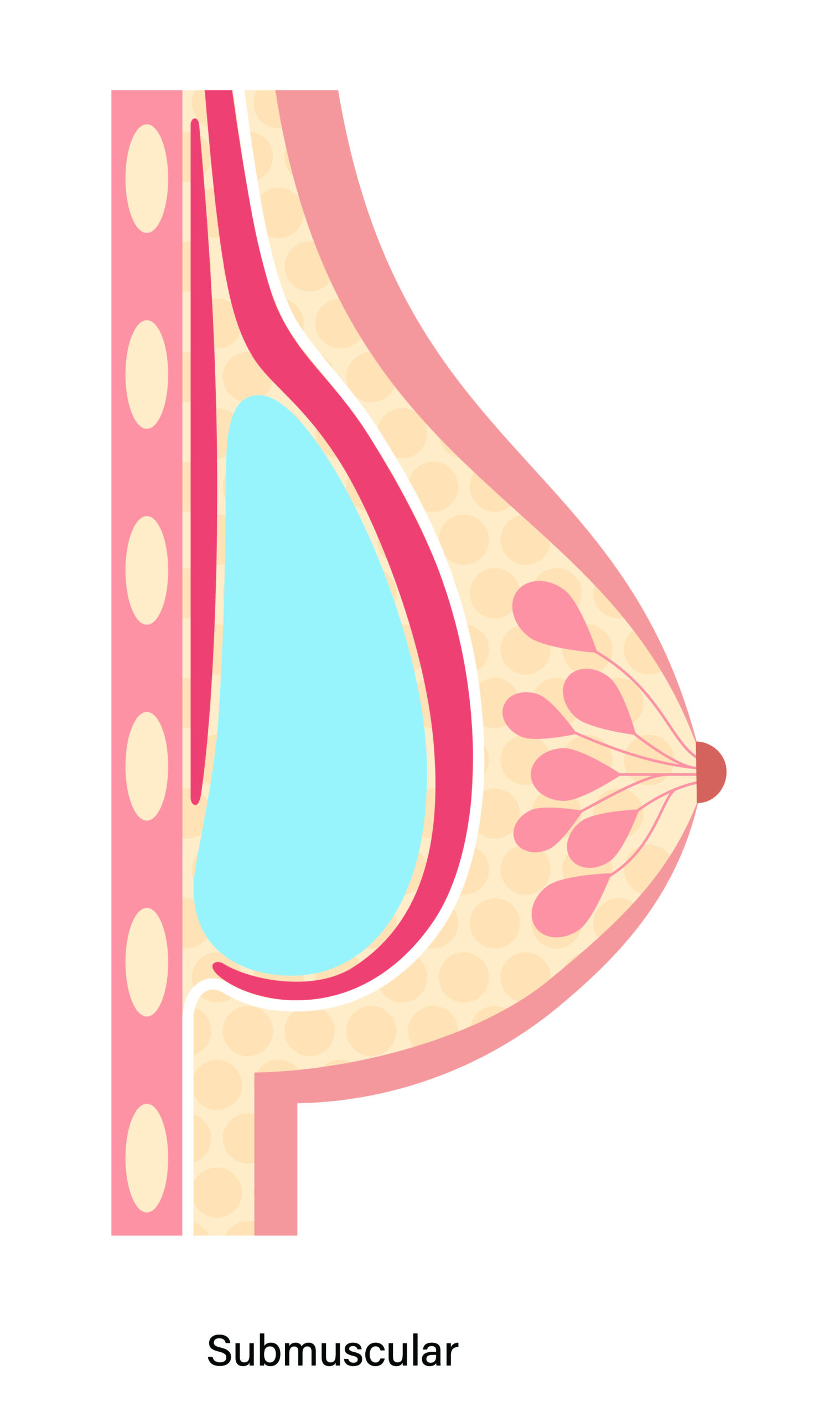
2. Sub-muscular placement
Because of the problems with implant visibility in the sub-glandular plane, surgeons developed techniques to place the implant under the pectoralis major muscle and thereby providing increased tissue coverage for the implants. This additional coverage can contribute to a more natural appearance and feel, especially for women with minimal breast tissue. The muscle acts as a cushion, reducing the risk of visible rippling or implant palpability.
However, the original description of this placement involved creating a small entrance to the plane beneath the muscle and squeezing the implant into this space. Because the muscle attachment to the chest wall restricted the implant movement from filling out the lower part of the breast, it often ended up very high and almost separate to the breast. For this reason, purely sub-muscular placement has largely been abandoned in the modern era, and when surgeons talk about sub-muscular placement, they more accurately mean releasing the lower part of the muscle to create a dual plane or bi-planar pocket for the implant.
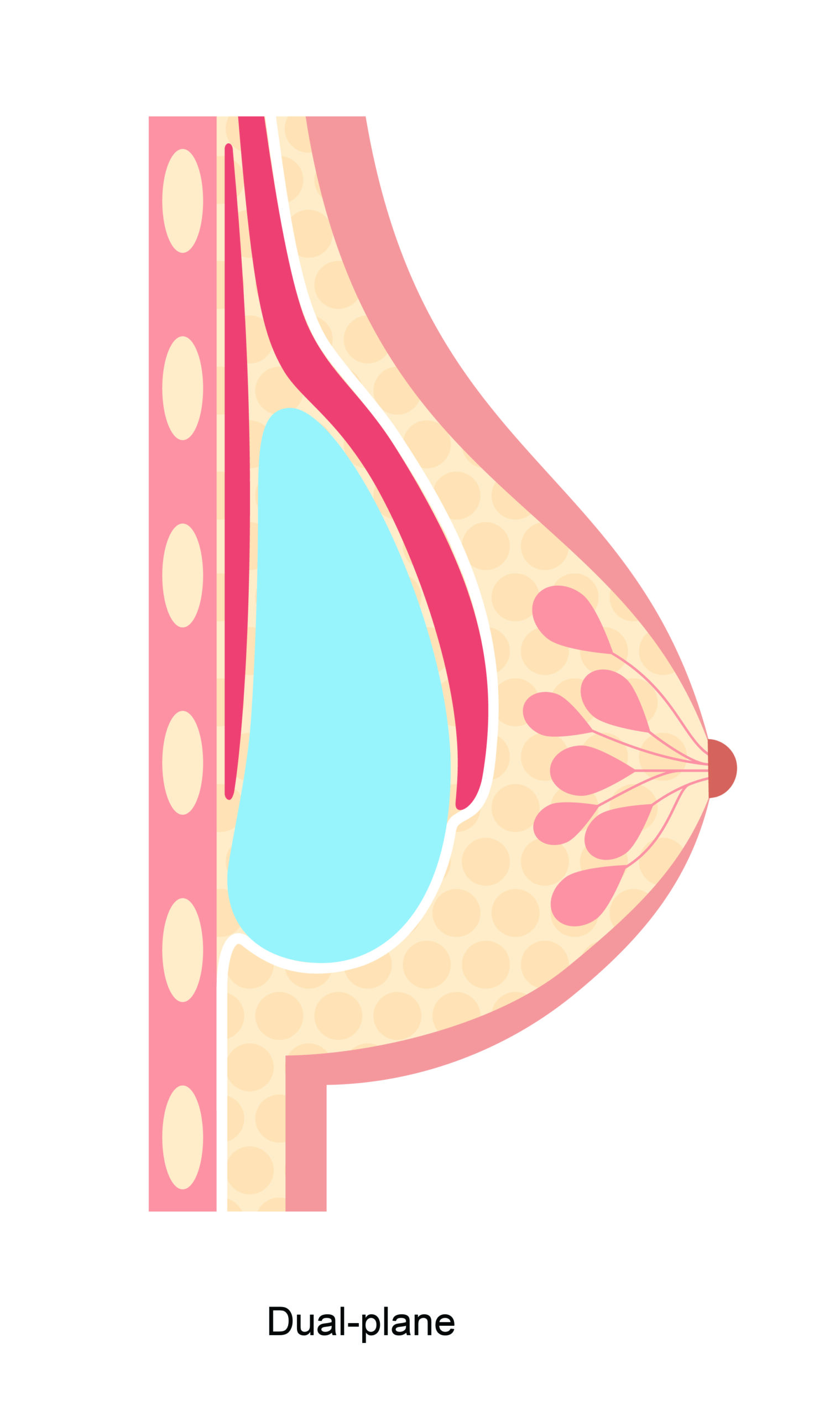
3. Dual plane or bi-planar placement
The dual plane pocket was first described by a very famous surgeon called John Tebbetts, from Texas. He described both releasing the breast tissue off the muscle, and then releasing the lower part of the muscle from the chest wall. This allows the muscle to ride up slightly and the implant is then covered by the muscle in the upper most part and the breast gland in the lower part – hence dual or two planes. There are some variations on this by splitting the muscle slightly higher up to change the amount of implant covered by the muscle and breast gland. These alternatives are often known as bi-planar.
The main advantage of a dual plane or bi-planar technique is that the upper part of the implant, which is usually visible above the bra, is covered by additional muscle tissue and the problem of implant edge visibility and rippling is diminished. Yet, the lower part is not restricted by the muscle. Hence, it’s an attempt to secure the advantages of both the sub-muscular placement and the sub-glandular placement combined.
Because the pectoralis muscle is attached to the breast bone or sternum in the cleavage area of the chest, implants placed deep to the muscle are limited in how far they can be brought together to enhance this cleavage area. Thus, dual plane breast augmentation can sometimes create breasts with a relatively large gap in the central chest. Release of the muscle in the lower portion can also create some visible notching in this area, so careful surgical dissection is essential.

John Tebbetts published this groundbreaking work in 2001. He demonstrated superb results from the dual plane technique but only with smooth surfaced implants. Textured surface implants do not act in the same way when placed underneath the muscle

Sub-muscular implant placement demonstrating widened and notched cleavage from poor surgical technique and decision making
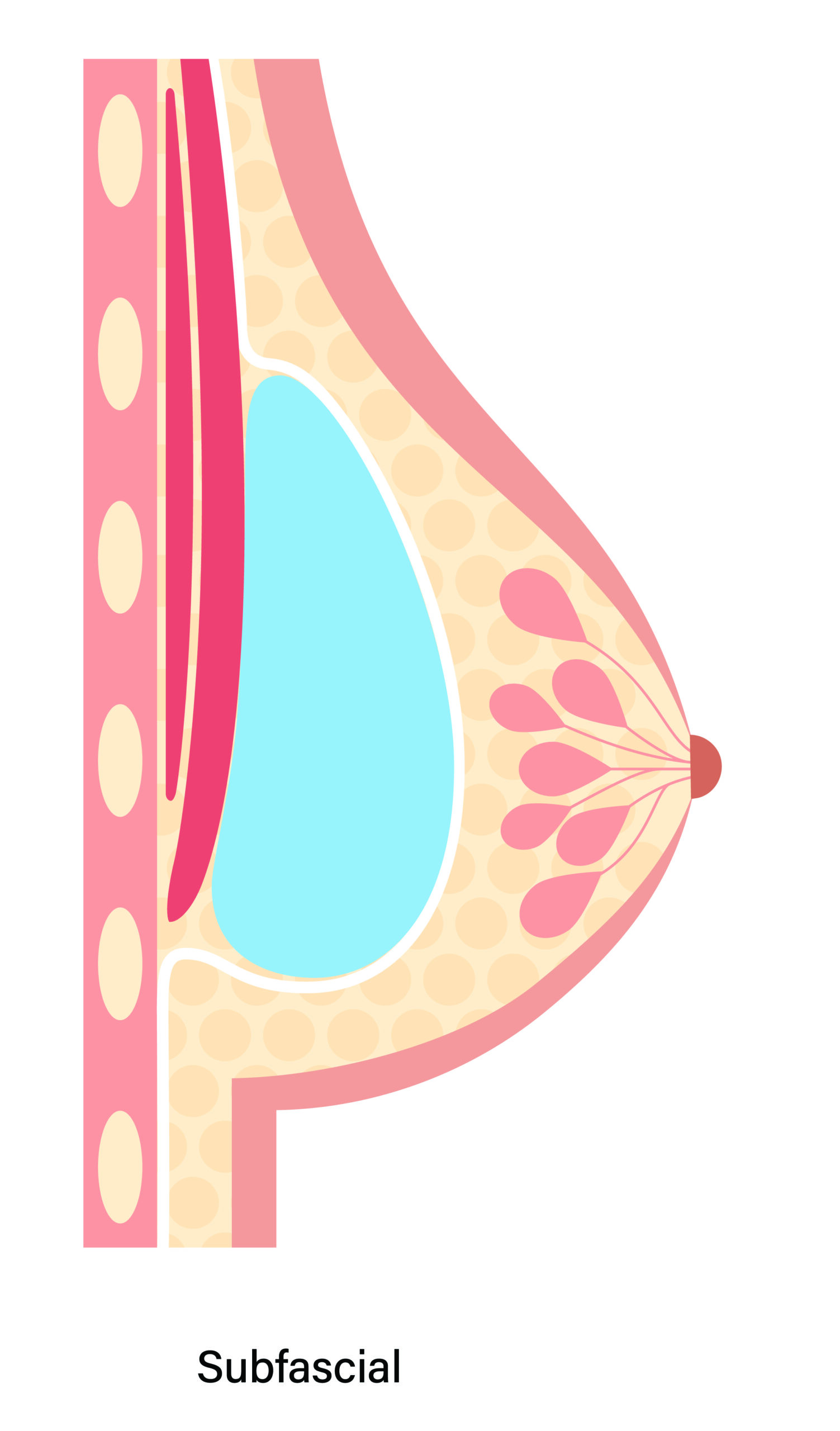
4. Sub-fascial placement
On the front surface of the pectoralis muscle there is a very thin layer of fascia (protective connective tissue covering) that separates the muscle from the breast tissue. This layer can be used to cover breast implants and separate the implant from the breast tissue.
Sub-fascial implant placement has gained popularity in recent years due to its potential advantages, which include:
Natural Results: Sub-fascial augmentation aims to provide a more natural-looking result compared to other placement options like sub-muscular or sub-glandular. Placing the implant beneath the fascia can help the implant’s edges blend more seamlessly with the surrounding tissues, resulting in a smoother, more natural contour.
Reduced Animation Deformity: As mentioned above, in sub-muscular placement, implants can move when the chest muscles are contracted, leading to animation deformity, where the breasts appear distorted during certain movements. Sub-fascial placement may reduce this effect since the implant is not directly under the muscle.
Less Postoperative Pain: Some patients report less postoperative discomfort and pain with sub-fascial placement compared to sub-muscular placement. This may be attributed to the fact that the chest muscles are not lifted or stretched as much during surgery.
Faster Recovery: Because the chest muscles are not manipulated as extensively, recovery time may be shorter, when compared with sub-muscular placement. Patients might experience less muscle-related soreness and may be able to resume their regular activities sooner.
Less Interference with Muscle Function: Sub-fascial placement involves minimal disruption of the chest muscles. This can be particularly beneficial for active individuals, athletes, or those who rely heavily on their chest muscles for work or daily activities.
Less Risk of Implant Distortion: In sub-muscular placement, the constant contraction and movement of the chest muscles can potentially lead to implant distortion or displacement over time. Sub-fascial placement may reduce this risk since the muscle’s actions have less impact on the implant’s position.
Potentially Reduced Risk of Capsular Contracture: Capsular contracture is a complication that can occur when scar tissue forms around the implant, causing the breast to become firm and distorted. Some studies suggest that sub-fascial placement might have a lower risk of capsular contracture compared to sub-glandular placement.
Sub-fascial placement therefore can provide many of the benefits of sub-muscular placement without the disruption to the muscle itself, whilst giving greater coverage compared to sub-glandular placement. Positioning implants beneath the pectoralis fascia can however be a more technically challenging operation in some patients, but clearly there are many advantages to this recent development in aesthetic breast surgery.
My own journey and understanding some of the problems that I see
When I first became a consultant plastic surgeon in 2004, I think it fair to say that like most surgeons of the time, I was a ‘Tebbetts devotee’. By this I mean that all of the senior surgeons that I worked with recommended the dual plane technique and I too believed this provided the most reliable option for almost all of my patients. However, I think that as a speciality we failed to recognise the significance of implant surface on the longer-term results. In the United States, for historical reasons related to the FDA moratorium of breast implants in the 1990s, over 95% of the breast implants used are smooth surfaced. In contrast, outside of the United States almost the opposite has been true, with textured implants predominating. (N.B. With the recent discovery of ALCL related to some textured surfaced implants the proportion of smooth surfaced implants around the World has increased.)
Under the muscle, smooth and textured surfaced implants perform very differently. Smooth implants are quite mobile and in the dual plane technique they fill out the breast fully. Textured implants however, tend to adhere to the surrounding tissue. Over time, when textured implants are placed behind the muscle, they tend to rise higher on the chest wall. When this is coupled with ageing of the breast tissue leading to descent of the breast tissue, this produces a high riding implant and drooped breast. This abnormally elongated shape of the breast is known as a Waterfall deformity or Snoopy breast.
The Waterfall deformity is a common problem that I see in patients with textured implants placed in a sub-muscular or dual plane position, and given this has been the predominant technique in the United Kingdom since the 1990s, correction of this problem occupies a significant proportion of my current practice. Added to this, many of my patients are now very active in the gym and they are likely to notice the loss of function associated with release of the muscle from the chest wall to allow the implants to be inserted into this position.
I believe it essential to make an individual patient assessment and recommend the most appropriate implant in the most appropriate position for that patient. However, where possible after an assessment of the soft tissue in the upper part of the breast, I now prefer sub-fascial placement for most patients requesting textured implants (this includes shaped implants which are all textured). For many patients, I also like to combine this with some fat transfer in a composite breast augmentation technique. If patients prefer to have a round, smooth surfaced implant, then because of the higher capsular contracture rate in front of the muscle, I will still use a dual-plane technique. Hence, Tebbetts was right all those years ago but only for smooth surfaced implants!

Sub-muscular textured implant placement often rides high over time with breast tissue descent causing a Waterfall or Snoopy deformity
Summary
The placement of breast implants relative to the pectoral muscles is a critical consideration in breast augmentation surgery. Each placement option, whether sub-muscular, sub-glandular, dual-plane or sub-fascial, has its advantages and considerations. Sub-muscular placement, including dual plane, offers increased tissue coverage but may involve a more extended recovery period and animation deformity. Over time, textured implants in this position tend to ride high and can lead to a Waterfall deformity. Sub-glandular placement may result in a quicker recovery and enhanced upper pole fullness but is associated with the risk of visible implant rippling. Sub-fascial placement, particularly when combined with fat transfer (composite breast augmentation) has the advantages of both methods for a customised approach in many patients and is currently my preferred technique. Consultation with a qualified plastic surgeon is crucial in determining the best implant placement option based on individual factors, to ensure optimal results and patient satisfaction.